Bursitis Of The Foot Treatment Solution
Overview
Heel bursitis is specifically the inflammation of the retrocalcaneal bursa, located at the back of the heel, under the Achilles tendon. There are a handful of factors that put you at risk for developing heel bursitis. Long distance runners are prone to heel bursitis, due to repeated stress and pounding upon the heel joint. Engaging in activities such as running, bicycling, walking, jumping, and stair climbing for extended periods of time can overwork the heel joints and start to irritate the bursae. Suddenly changing to a high-intensity workout regime puts a lot of stress on the heel, making it vulnerable to injury. Hard blows/bumps to the heel can immediately damage the bursae, leading to swelling and inflammation. Training at high intensities without stretching and warming up can also contribute to the development of heel bursitis. Even improper footwear can be a big factor. Some other conditions can put you at risk as well, such as: tarsal tunnel syndrome, rheumatoid arthritis, plantar fasciitis, muscle weakness, joint stiffness, and heel spurs. It is very important to get a professional diagnosis if you are having heel pain because heel bursitis is often confused for Achilles tendonitis, and the proper treatments are very different. The pain could also be plantar fasciitis or general heel pain syndrome.
Causes
Causes of bursitis can be from any form of friction between bone and the soft tissues. The most common cause is due to abnormal pronation.
Symptoms
Your heel may feel more sensitive to the cold and ache in cold and damp weather due to impaired circulation. These symptoms are often the result of failure to treat the injury properly from the outset and overicing.
Diagnosis
To begin with, your doctor will gather a medical history about you and your current condition and symptoms. He/she will inquire about the level of your heel pain, the how long you have had the symptoms and the limitations you are experiencing. Details about what and when the pain started, all are very helpful in providing you with a diagnoses of your ankle / heel.
Non Surgical Treatment
Over-the-counter or custom heel wedges may help to decrease the stress placed on the attachment of the achilles tendon and the associated bursa. If these interventions are ineffective, then some health care providers may inject a small amount of steroids into the bursa. If the condition is associated with Achilles tendonitis, then casting the ankle to prevent motion for several weeks can be effective. Very rarely, surgery may be necessary to remove the inflamed bursa.
Surgical Treatment
Surgery is rarely done strictly for treatment of a bursitis. If any underlying cause is the reason, this may be addressed surgically. During surgery for other conditions, a bursa may be seen and removed surgically.
Heel bursitis is specifically the inflammation of the retrocalcaneal bursa, located at the back of the heel, under the Achilles tendon. There are a handful of factors that put you at risk for developing heel bursitis. Long distance runners are prone to heel bursitis, due to repeated stress and pounding upon the heel joint. Engaging in activities such as running, bicycling, walking, jumping, and stair climbing for extended periods of time can overwork the heel joints and start to irritate the bursae. Suddenly changing to a high-intensity workout regime puts a lot of stress on the heel, making it vulnerable to injury. Hard blows/bumps to the heel can immediately damage the bursae, leading to swelling and inflammation. Training at high intensities without stretching and warming up can also contribute to the development of heel bursitis. Even improper footwear can be a big factor. Some other conditions can put you at risk as well, such as: tarsal tunnel syndrome, rheumatoid arthritis, plantar fasciitis, muscle weakness, joint stiffness, and heel spurs. It is very important to get a professional diagnosis if you are having heel pain because heel bursitis is often confused for Achilles tendonitis, and the proper treatments are very different. The pain could also be plantar fasciitis or general heel pain syndrome.
Causes
Causes of bursitis can be from any form of friction between bone and the soft tissues. The most common cause is due to abnormal pronation.
Symptoms
Your heel may feel more sensitive to the cold and ache in cold and damp weather due to impaired circulation. These symptoms are often the result of failure to treat the injury properly from the outset and overicing.
Diagnosis
To begin with, your doctor will gather a medical history about you and your current condition and symptoms. He/she will inquire about the level of your heel pain, the how long you have had the symptoms and the limitations you are experiencing. Details about what and when the pain started, all are very helpful in providing you with a diagnoses of your ankle / heel.
Non Surgical Treatment
Over-the-counter or custom heel wedges may help to decrease the stress placed on the attachment of the achilles tendon and the associated bursa. If these interventions are ineffective, then some health care providers may inject a small amount of steroids into the bursa. If the condition is associated with Achilles tendonitis, then casting the ankle to prevent motion for several weeks can be effective. Very rarely, surgery may be necessary to remove the inflamed bursa.
Surgical Treatment
Surgery is rarely done strictly for treatment of a bursitis. If any underlying cause is the reason, this may be addressed surgically. During surgery for other conditions, a bursa may be seen and removed surgically.
New Hammer Toe Treatment
 Overview
Overview
Hammertoes are another forefoot deformity that can take a walker out of their activity. A hammertoe generally represent a tendon imbalance in the toes caused by one of the toe tendons getting an advantage over another toe tendon. Most commonly, it is one or all of the long extensor tendons on the top of the foot that gets an advantage over one or all of the flexor tendons on the bottom of the foot, to cause the first joint in the toe to be elevated above the ground. Most shoe wearing people chronically alter the delicate balance that co-exists amongst the toe tendons whether they know it or not.
Causes
Hammer toe is often caused by wearing shoes that do not fit properly. If shoes are too small either in length or width, then the toes are held in a shortened position for long periods and the muscles eventually shorten and pull the toes into the bent position. Alternatively it can be caused by overactivity in the extensor digitorum dongus muscle (right) and a weakness in the counteracting muscle under the foot, such as flexor digitorum longus. Sometimes it can be a congenital condition, meaning it is present from birth. It is also more common in those with arthritis in the foot or diabetes.
 Symptoms
Symptoms
A hammer toe may be painful, especially when irritated by a shoe. All four toe conditions may cause cramps in the toes, foot and leg due to the abnormal function of the tendons in the foot. If a mallet toe has occurred, you are likely to suffer from a corn at the end of the toe. A hammertoe may cause a corn on the top of the toe. Infections and ulcers can also occur. In severe cases a mallet toe, trigger toe, claw toe or a hammer toe may create a downward pressure on the foot, which can result in hard skin and corns on the soles of the feet.
Diagnosis
A hammertoe is usually diagnosed with a physical inspection of your toe. Imaging tests, such as X-rays, may be ordered if you have had a bone, muscle, or ligament injury in your toe.
Non Surgical Treatment
Any forefoot problems that cause pain or discomfort should be given prompt attention. Ignoring the symptoms can aggravate the condition and lead to a breakdown of tissue, or possibly even infection. Conservative treatment of mallet toes begins with accommodating the deformity. The goal is to relieve pressure, reduce friction, and transfer forces from the sensitive areas. Shoes with a high and broad toe box (toe area) are recommended for people suffering from forefoot deformities such as mallet toes. This prevents further irritation in the toe area from developing. Other conservative treatment includes forefoot supports such as gel toe caps, gel toe shields and toe crests. Gel forefoot supports provide immediate comfort and relief from common forefoot disorders without drying the skin.
Surgical Treatment
In some cases, usually when the hammertoe has become more rigid and painful, or when an open sore has developed, surgery is needed. Often patients with hammertoe have bunions or other foot deformities corrected at the same time. In selecting the procedure or combination of procedures for your particular case, the foot and ankle surgeon Hammer toe will take into consideration the extent of your deformity, the number of toes involved, your age, your activity level, and other factors. The length of the recovery period will vary, depending on the procedure or procedures performed.
The Truth Related To Over-Pronation Of The Foot
Overview
Overpronation still continues to be misused and misunderstood. For example, there was a study that got a lot of recent mileage in the mainstream media and the blogosphere that claimed to show that foot pronation was not associated with injury risk. It was intriguing following comments on the study in mainstream media and in social media, especially the parroting of the press release without any critical appraisal. The study actually eliminated the ?overpronators? that were probably at high risk from the study then found that ?overpronation? was not a risk factor. What is more intriguing was that there was another study from around the same time that found the exact opposite. Clearly, the data on ?overpronation? and risk for injury in runners is mixed, so we need to rely on the more formal systematic reviews and meta-analyses of all the data. The most recent one of those concluded that ?overpronation? is just a small risk factor for running injury risk, but it is still statistically significant.
Causes
Pronation can occur as an overuse syndrome in active runners, where a great deal of stress is placed on ligaments and tendons that support the medial column. Obesity is another predictor for pronation and deterioration of the medial ligaments and posterior tibial tendon due to excessive stress on these tissues. Acute Trauma can also lead to over-pronation when ligaments are torn or tendon is ruptured. Once again this can lead to a collapse of the medial column. Arthritic conditions involving the knee joint when the joint is in varus (inner collapse) posture, this places the center of gravity over the ankle joint rather than the foot causing undue pressure on the inner ankle.
Symptoms
Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven.
Diagnosis
To easily get an idea of whether a person overpronates, look at the position and condition of certain structures in the feet and ankles when he/she stands still. When performing weight-bearing activities like walking or running, muscles and other soft tissue structures work to control gravity's effect and ground reaction forces to the joints. If the muscles of the leg, pelvis, and feet are working correctly, then the joints in these areas such as the knees, hips, and ankles will experience less stress. However, if the muscles and other soft tissues are not working efficiently, then structural changes and clues in the feet are visible and indicate habitual overpronation.
Non Surgical Treatment
If you overpronate, you should talk with a foot and ankle specialist, especially if symptoms have not developed yet. Questions you may want to ask your doctor include what are the best running shoes on the market? Where can I find those shoes? If over-the-counter orthotics don?t work, how long should I wait before contacting you for custom-made orthotics? On my next visit, what type of diagnostic testing should I expect? If I limit the amount of time I spend running, will my overpronation symptoms disappear? What additional treatment options can we try?
Prevention
Wear supportive shoes. If we're talking runners you're going to fall in the camp of needing 'motion control' shoes or shoes built for 'moderate' or 'severe' pronators. There are many good brands of shoes out there. Don't just wear these running, the more often the better. Make slow changes. Sudden changes in your training will aggravate your feet more than typical. Make sure you slowly increase your running/walking distance, speed and even how often you go per week. Strengthen your feet. As part of your running/walking warm up or just as part of a nightly routine try a few simple exercises to strengthen your feet, start with just ten of each and slowly add more sets and intensity. Stand facing a mirror and practice raising your arch higher off the ground without lifting your toes. Sit with a towel under your feet, scrunch your toes and try to pull the towel in under your feet. Sitting again with feet on the ground lift your heels as high as you can, then raise and lower on to toe tips.
Overpronation still continues to be misused and misunderstood. For example, there was a study that got a lot of recent mileage in the mainstream media and the blogosphere that claimed to show that foot pronation was not associated with injury risk. It was intriguing following comments on the study in mainstream media and in social media, especially the parroting of the press release without any critical appraisal. The study actually eliminated the ?overpronators? that were probably at high risk from the study then found that ?overpronation? was not a risk factor. What is more intriguing was that there was another study from around the same time that found the exact opposite. Clearly, the data on ?overpronation? and risk for injury in runners is mixed, so we need to rely on the more formal systematic reviews and meta-analyses of all the data. The most recent one of those concluded that ?overpronation? is just a small risk factor for running injury risk, but it is still statistically significant.
Causes
Pronation can occur as an overuse syndrome in active runners, where a great deal of stress is placed on ligaments and tendons that support the medial column. Obesity is another predictor for pronation and deterioration of the medial ligaments and posterior tibial tendon due to excessive stress on these tissues. Acute Trauma can also lead to over-pronation when ligaments are torn or tendon is ruptured. Once again this can lead to a collapse of the medial column. Arthritic conditions involving the knee joint when the joint is in varus (inner collapse) posture, this places the center of gravity over the ankle joint rather than the foot causing undue pressure on the inner ankle.
Symptoms
Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven.
Diagnosis
To easily get an idea of whether a person overpronates, look at the position and condition of certain structures in the feet and ankles when he/she stands still. When performing weight-bearing activities like walking or running, muscles and other soft tissue structures work to control gravity's effect and ground reaction forces to the joints. If the muscles of the leg, pelvis, and feet are working correctly, then the joints in these areas such as the knees, hips, and ankles will experience less stress. However, if the muscles and other soft tissues are not working efficiently, then structural changes and clues in the feet are visible and indicate habitual overpronation.
Non Surgical Treatment
If you overpronate, you should talk with a foot and ankle specialist, especially if symptoms have not developed yet. Questions you may want to ask your doctor include what are the best running shoes on the market? Where can I find those shoes? If over-the-counter orthotics don?t work, how long should I wait before contacting you for custom-made orthotics? On my next visit, what type of diagnostic testing should I expect? If I limit the amount of time I spend running, will my overpronation symptoms disappear? What additional treatment options can we try?
Prevention
Wear supportive shoes. If we're talking runners you're going to fall in the camp of needing 'motion control' shoes or shoes built for 'moderate' or 'severe' pronators. There are many good brands of shoes out there. Don't just wear these running, the more often the better. Make slow changes. Sudden changes in your training will aggravate your feet more than typical. Make sure you slowly increase your running/walking distance, speed and even how often you go per week. Strengthen your feet. As part of your running/walking warm up or just as part of a nightly routine try a few simple exercises to strengthen your feet, start with just ten of each and slowly add more sets and intensity. Stand facing a mirror and practice raising your arch higher off the ground without lifting your toes. Sit with a towel under your feet, scrunch your toes and try to pull the towel in under your feet. Sitting again with feet on the ground lift your heels as high as you can, then raise and lower on to toe tips.
What Would Cause Severs Disease?
Overview
Sever's disease, also known as calcaneal apophysitis, is a medical condition that causes heel pain in one or both feet of children during the period when their feet are growing. Sever's disease occurs most commonly in boys and girls between the ages of 8 and 14 years of age. Sever's disease occurs when the part of the child's heel known as the growth plate, or the calcaneal epiphysis, an area attached to the Achilles tendon, suffers an injury or when the muscles and tendons of the growing foot do not keep pace with bone growth. The result is constant pain experienced at the back of the heel and the inability to put any weight on the heel, forcing the child to bear weight on their toes while walking. A toe gait develops in which the child must change the way they walk to avoid placing weight on the painful heel, a position that can lead to other developmental problems.
Causes
The cause of Sever's disease is not entirely clear. It is most likely due to overuse or repeated minor trauma that happens in a lot of sporting activities - the cartilage join between the two parts of the bone can not take all the shear stress of the activities. Some children seem to be just more prone to it for an unknown reason - combine this with sport, especially if its on a hard surface and the risk of getting it increases. It can be almost epidemic at the start of some sports seasons, especially winter. At the start of winter, the grounds are often harder, but soften later. Children who are heavier are also at greater risk for developing calcaneal apophysitis.
Symptoms
The most prominent symptom of Sever's disease is heel pain which is usually aggravated by physical activity such as walking, running or jumping. The pain is localised to the posterior and plantar side of the heel over the calcaneal apophysis. Sometimes, the pain may be so severe that it may cause limping and interfere with physical performance in sports. External appearance of the heel is almost always normal, and signs of local disease such as edema, erythema (redness) are absent. The main diagnostic tool is pain on medial- lateral compression of the calcaneus in the area of growth plate, so called squeeze test. Foot radiographs are usually normal. Therefore the diagnosis of Sever's disease is primarily clinical.
Diagnosis
Physical examination varies depending on the severity and length of involvement. Bilateral involvement is present in approximately 60% of cases. Most patients experience pain with deep palpation at the Achilles insertion and pain when performing active toe raises. Forced dorsiflexion of the ankle also proves uncomfortable and is relieved with passive equinus positioning. Swelling may be present but usually is mild. In long-standing cases, the child may have calcaneal enlargement.
Non Surgical Treatment
Rest is best to allow healing .Only do as much exercise as able without causing pain. Many children can continue to play sports but if pain is severe then stopping the activity may be the only way to allow the pain to settle. The child might be able to do things that do not put pressure on the heel, such as swimming and cycling. Ice and cold therapy may be useful to reduce pain and swelling, particularly following activity or sport. The area should be iced until it feels cold not ?frozen?. Never apply ice directly onto the skin, as this may cause tissue damage. Medication. The following will help treat your child?s pain. Paracetamol (see bottle for instructions) Ibuprofen (see bottle for instructions). Exercises, perform foot and leg exercises to stretch and strengthen the leg muscles & tendons. Increase calf flexibility by doing calf stretches several times per day. Protect the heel, your shoes might need a heel lift or arch support. Select a shoe with good arch support and heel lift if possible. Take it one step at a time: gradually resume running and impact activities as symptoms allow.
Prevention
Can Calcaneal Apophysitis Be Prevented? The chances of a child developing heel pain can be reduced by avoiding obesity. Choosing well-constructed, supportive shoes that are appropriate for the child?s activity. Avoiding or limiting wearing of cleated athletic shoes. Avoiding activity beyond a child?s ability.
Sever's disease, also known as calcaneal apophysitis, is a medical condition that causes heel pain in one or both feet of children during the period when their feet are growing. Sever's disease occurs most commonly in boys and girls between the ages of 8 and 14 years of age. Sever's disease occurs when the part of the child's heel known as the growth plate, or the calcaneal epiphysis, an area attached to the Achilles tendon, suffers an injury or when the muscles and tendons of the growing foot do not keep pace with bone growth. The result is constant pain experienced at the back of the heel and the inability to put any weight on the heel, forcing the child to bear weight on their toes while walking. A toe gait develops in which the child must change the way they walk to avoid placing weight on the painful heel, a position that can lead to other developmental problems.
Causes
The cause of Sever's disease is not entirely clear. It is most likely due to overuse or repeated minor trauma that happens in a lot of sporting activities - the cartilage join between the two parts of the bone can not take all the shear stress of the activities. Some children seem to be just more prone to it for an unknown reason - combine this with sport, especially if its on a hard surface and the risk of getting it increases. It can be almost epidemic at the start of some sports seasons, especially winter. At the start of winter, the grounds are often harder, but soften later. Children who are heavier are also at greater risk for developing calcaneal apophysitis.
Symptoms
The most prominent symptom of Sever's disease is heel pain which is usually aggravated by physical activity such as walking, running or jumping. The pain is localised to the posterior and plantar side of the heel over the calcaneal apophysis. Sometimes, the pain may be so severe that it may cause limping and interfere with physical performance in sports. External appearance of the heel is almost always normal, and signs of local disease such as edema, erythema (redness) are absent. The main diagnostic tool is pain on medial- lateral compression of the calcaneus in the area of growth plate, so called squeeze test. Foot radiographs are usually normal. Therefore the diagnosis of Sever's disease is primarily clinical.
Diagnosis
Physical examination varies depending on the severity and length of involvement. Bilateral involvement is present in approximately 60% of cases. Most patients experience pain with deep palpation at the Achilles insertion and pain when performing active toe raises. Forced dorsiflexion of the ankle also proves uncomfortable and is relieved with passive equinus positioning. Swelling may be present but usually is mild. In long-standing cases, the child may have calcaneal enlargement.
Non Surgical Treatment
Rest is best to allow healing .Only do as much exercise as able without causing pain. Many children can continue to play sports but if pain is severe then stopping the activity may be the only way to allow the pain to settle. The child might be able to do things that do not put pressure on the heel, such as swimming and cycling. Ice and cold therapy may be useful to reduce pain and swelling, particularly following activity or sport. The area should be iced until it feels cold not ?frozen?. Never apply ice directly onto the skin, as this may cause tissue damage. Medication. The following will help treat your child?s pain. Paracetamol (see bottle for instructions) Ibuprofen (see bottle for instructions). Exercises, perform foot and leg exercises to stretch and strengthen the leg muscles & tendons. Increase calf flexibility by doing calf stretches several times per day. Protect the heel, your shoes might need a heel lift or arch support. Select a shoe with good arch support and heel lift if possible. Take it one step at a time: gradually resume running and impact activities as symptoms allow.
Prevention
Can Calcaneal Apophysitis Be Prevented? The chances of a child developing heel pain can be reduced by avoiding obesity. Choosing well-constructed, supportive shoes that are appropriate for the child?s activity. Avoiding or limiting wearing of cleated athletic shoes. Avoiding activity beyond a child?s ability.
Cure For Flat Feet In Adults
Overview
Flatfoot may sound like a characteristic of a certain water animal rather than a human problem. Flatfoot is a condition in which the arch of the foot is fallen and the foot is pointed outward. In contrast to a flatfoot condition that has always been present, this type develops after the skeleton has reached maturity. There are several situations that can result in fallen arches, including fracture, dislocation, tendon laceration, tarsal coalition, and arthritis. One of the most common conditions that can lead to this foot problem is posterior tibial tendon dysfunction. The posterior tibial tendon attaches the calf muscle to the bones on the inside of the foot and is crucial in holding up and supporting the arch. An acute injury or overuse can cause this tendon to become inflamed or even torn, and the arch of the foot will slowly fall over time. 
Causes
There are multiple factors contributing to the development of this problem. Damage to the nerves, ligaments, and/or tendons of the foot can cause subluxation (partial dislocation) of the subtalar or talonavicular joints. Bone fracture is a possible cause. The resulting joint deformity from any of these problems can lead to adult-acquired flatfoot deformity. Dysfunction of the posterior tibial tendon has always been linked with adult-acquired flatfoot deformity (AAFD). The loss of active and passive pull of the tendon alters the normal biomechanics of the foot and ankle. The reasons for this can be many and varied as well. Diabetes, high blood pressure, and prolonged use of steroids are some of the more common causes of adult-acquired flatfoot deformity (AAFD) brought on by impairment of the posterior tibialis tendon. Overstretching or rupture of the tendon results in tendon and muscle imbalance in the foot leading to adult-acquired flatfoot deformity (AAFD). Rheumatoid arthritis is one of the more common causes. About half of all adults with this type of arthritis will develop adult flatfoot deformity over time. In such cases, the condition is gradual and progressive. Obesity has been linked with this condition. Loss of blood supply for any reason in the area of the posterior tibialis tendon is another factor. Other possible causes include bone fracture or dislocation, a torn or stretched tendon, or a neurologic condition causing weakness.
Symptoms
Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot.
Diagnosis
Perform a structural assessment of the foot and ankle. Check the ankle for alignment and position. When it comes to patients with severe PTTD, the deltoid has failed, causing an instability of the ankle and possible valgus of the ankle. This is a rare and difficult problem to address. However, if one misses it, it can lead to dire consequences and potential surgical failure. Check the heel alignment and position of the heel both loaded and during varus/valgus stress. Compare range of motion of the heel to the normal contralateral limb. Check alignment of the midtarsal joint for collapse and lateral deviation. Noting the level of lateral deviation in comparison to the contralateral limb is critical for surgical planning. Check midfoot alignment of the naviculocuneiform joints and metatarsocuneiform joints both for sag and hypermobility.
Non surgical Treatment
A painless flatfoot that does not hinder your ability to walk or wear shoes requires no special treatment or orthotic device. Other treatment options depend on the cause and progression of the flatfoot. Conservative treatment options include making shoe modifications. Using orthotic devices such as arch supports and custom-made orthoses. Taking nonsteroidal anti-inflammatory drugs such as ibuprofen to relieve pain. Using a short-leg walking cast or wearing a brace. Injecting a corticosteroid into the joint to relieve pain. Rest and ice. Physical therapy. In some cases, surgery may be needed to correct the problem. Surgical procedures can help reduce pain and improve bone alignment. 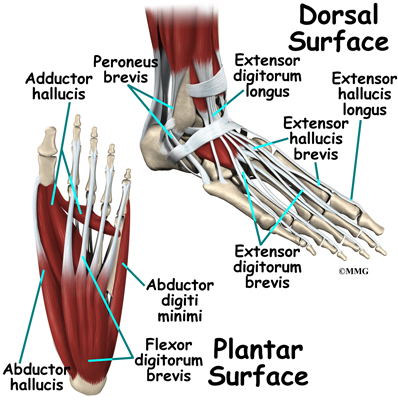
Surgical Treatment
Flatfoot reconstruction (osteotomy). This is often recommended for flexible flatfoot condition. Flatfoot reconstruction involves cutting and shifting the heel bone into a more neutral position, transferring the tendon used to flex the lesser toes (all but the big toe) to strengthen the posterior tibial tendon, and lengthening the calf muscle. Fusion (also known as triple arthrodesis). Fusion involves fusing, or making stiff, three joints in the back of the foot the subtalar, talonavicular, and calcaneocuboid joints, to realign the foot and give it a more natural shape. Pins or screws hold the area in place until it heals. Fusion is often recommended for a rigid flatfoot deformity or evidence of arthritis. Both of these surgeries can provide excellent pain relief and correction.
What Can cause Adult Aquired FlatFoot ?
Overview
Adult-acquired flatfoot is a challenging condition to treat. It is defined as a symptomatic, progressive deformity of the foot caused by loss of supportive structures of the medial arch. It is becoming increasingly frequent with the aging population and the obesity epidemic. Patients commonly try to lose weight by exercising to improve the condition. This often leads to worsening of symptoms and progression of the disorder. Early recognition of this complex disorder is essential, if chronic pain and surgery are to be avoided.
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot. Sometimes this can be a result of specific trauma, but usually the tendon becomes injured from wear and tear over time. This is more prevalent in individuals with an inherited flat foot but excessive weight, age, and level of activity are also contributing factors.
Symptoms
Often, this condition is only present in one foot, but it can affect both. Adult acquired flatfoot symptoms vary, but can swelling of the foot's inner side and aching heel and arch pain. Some patients experience no pain, but others may experience severe pain. Symptoms may increase during long periods of standing, resulting in fatigue. Symptoms may change over time as the condition worsens. The pain may move to the foot's outer side, and some patients may develop arthritis in the ankle and foot.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Non-surgical treatment consists of custom orthoses and or special bracing devices along with supportive measures aimed at reducing the symptoms. While non-surgical treatment helps the majority of patients with PTTD, progressive cases may require surgical treatment including soft tissue tendon transfers, osteotomies and lastly fusion.

Surgical Treatment
If conservative treatments don?t work, your doctor may recommend surgery. Several procedures can be used to treat posterior tibial tendon dysfunction; often more than one procedure is performed at the same time. Your doctor will recommend a specific course of treatment based on your individual case. Surgical options include. Tenosynovectomy. In this procedure, the surgeon will clean away (debride) and remove (excise) any inflamed tissue surrounding the tendon. Osteotomy. This procedure changes the alignment of the heel bone (calcaneus). The surgeon may sometimes have to remove a portion of the bone. Tendon transfer: This procedure uses some fibers from another tendon (the flexor digitorum longus, which helps bend the toes) to repair the damaged posterior tibial tendon. Lateral column lengthening, In this procedure, the surgeon places a small wedge-shaped piece of bone into the outside of the calcaneus. This helps realign the bones and recreates the arch. Arthrodesis. This procedure welds (fuses) one or more bones together, eliminating movement in the joint. This stabilizes the hindfoot and prevents the condition from progressing further.
Adult-acquired flatfoot is a challenging condition to treat. It is defined as a symptomatic, progressive deformity of the foot caused by loss of supportive structures of the medial arch. It is becoming increasingly frequent with the aging population and the obesity epidemic. Patients commonly try to lose weight by exercising to improve the condition. This often leads to worsening of symptoms and progression of the disorder. Early recognition of this complex disorder is essential, if chronic pain and surgery are to be avoided.
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot. Sometimes this can be a result of specific trauma, but usually the tendon becomes injured from wear and tear over time. This is more prevalent in individuals with an inherited flat foot but excessive weight, age, and level of activity are also contributing factors.
Symptoms
Often, this condition is only present in one foot, but it can affect both. Adult acquired flatfoot symptoms vary, but can swelling of the foot's inner side and aching heel and arch pain. Some patients experience no pain, but others may experience severe pain. Symptoms may increase during long periods of standing, resulting in fatigue. Symptoms may change over time as the condition worsens. The pain may move to the foot's outer side, and some patients may develop arthritis in the ankle and foot.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Non-surgical treatment consists of custom orthoses and or special bracing devices along with supportive measures aimed at reducing the symptoms. While non-surgical treatment helps the majority of patients with PTTD, progressive cases may require surgical treatment including soft tissue tendon transfers, osteotomies and lastly fusion.
Surgical Treatment
If conservative treatments don?t work, your doctor may recommend surgery. Several procedures can be used to treat posterior tibial tendon dysfunction; often more than one procedure is performed at the same time. Your doctor will recommend a specific course of treatment based on your individual case. Surgical options include. Tenosynovectomy. In this procedure, the surgeon will clean away (debride) and remove (excise) any inflamed tissue surrounding the tendon. Osteotomy. This procedure changes the alignment of the heel bone (calcaneus). The surgeon may sometimes have to remove a portion of the bone. Tendon transfer: This procedure uses some fibers from another tendon (the flexor digitorum longus, which helps bend the toes) to repair the damaged posterior tibial tendon. Lateral column lengthening, In this procedure, the surgeon places a small wedge-shaped piece of bone into the outside of the calcaneus. This helps realign the bones and recreates the arch. Arthrodesis. This procedure welds (fuses) one or more bones together, eliminating movement in the joint. This stabilizes the hindfoot and prevents the condition from progressing further.
The Major Causes And Treatments Of Achilles Tendon Pain
Overview
 Achilles-tendinitis is characterized by inflammation and pain at the Achilles tendon (back of the ankle). This tendon, sometimes called the heel cord, is the tendon attachment of the calf muscles from the leg and knee to the heel. This structure is important in standing on your toes or in the pushing-off phase of walking, running, or jumping.Achilles-tendinitis is usually a grade 1 or 2 strain of the tendon. A grade 1 strain is a mild strain. There is a slight pull of the tendon without obvious tendon tearing. (There is microscopic tendon tearing.) There is no loss of strength, and the tendon is the correct length. A grade 2 strain is a moderate strain. There is tearing of tendon fibers within the substance of the tendon or where the tendon attaches to muscle or bone. The length of the tendon or whole muscle-tendon-bone unit is increased, and there is usually decreased strength. A grade 3 strain is a complete rupture of the tendon.
Achilles-tendinitis is characterized by inflammation and pain at the Achilles tendon (back of the ankle). This tendon, sometimes called the heel cord, is the tendon attachment of the calf muscles from the leg and knee to the heel. This structure is important in standing on your toes or in the pushing-off phase of walking, running, or jumping.Achilles-tendinitis is usually a grade 1 or 2 strain of the tendon. A grade 1 strain is a mild strain. There is a slight pull of the tendon without obvious tendon tearing. (There is microscopic tendon tearing.) There is no loss of strength, and the tendon is the correct length. A grade 2 strain is a moderate strain. There is tearing of tendon fibers within the substance of the tendon or where the tendon attaches to muscle or bone. The length of the tendon or whole muscle-tendon-bone unit is increased, and there is usually decreased strength. A grade 3 strain is a complete rupture of the tendon.
Causes
Although a specific incident of overstretching can cause an Achilles tendon disorder, these injuries typically result from a gradually progressive overload of the Achilles tendon or its attachment to bone. The cause of this chronic overload is usually a combination of factors that can put excess stress on the tendon: being overweight, having a tight calf muscle, standing or walking for a long period of time, wearing excessively stiff or flat footwear, or engaging in significant sports activity.
Symptoms
There are several types of Achilles tendinitis symptoms, but all of them are closely related. People who suffer from Achilles tendon pain typically have swelling in the Achilles tendon, and that pain can be chronic as the microscopic tears in the area become more prevalent over time. The most intense pain is typically located just a few centimeters above the area where the tendon meets the heel. This area is called the watershed zone, and the amount of blood moving through it is what gives it the highest potential for injury, especially for athletes. Most of the Achilles tendinitis symptoms in people with the condition will happen immediately after they have been inactive for a fairly significant amount of time. That means that the most pain will generally be felt after sitting or lying down for an extended period, or right after waking up in the morning and getting moving. If you aren?t positive that you are suffering specifically from Achilles tendinitis symptoms, consult a doctor to make sure.
Diagnosis
A doctor examines the patient, checking for pain and swelling along the posterior of the leg. The doctor interviews the patient regarding the onset, history, and description of pain and weakness. The muscles, tissues, bones, and blood vessels may be evaluated with imaging studies, such as X-ray, ultrasound, or MRI.
Nonsurgical Treatment
There are a variety of treatments for Achilles tendonitis. These range from rest and aspirin to steroid injections and surgery. Your doctor might suggest, reducing your physical activity, stretching and strengthening the calf muscles, switching to a different, less strenuous sport, icing the area after exercise or when in pain, raising your foot to decrease swelling, wearing a brace or compressive elastic bandage to prevent heel movement, undergoing physical therapy, taking anti-inflammatory medication (e.g., aspirin or ibuprofen) for a limited time, getting steroid injections, Sometimes more conservative treatments are not effective. In these cases, surgery may be necessary to repair the Achilles tendon. If the condition intensifies and is left untreated, there?s a greater risk of an Achilles rupture. This can cause sharp pain in the heel area.

Surgical Treatment
Surgery is considered when non-operative measures fail. Patient compliance and postoperative management is an important aspect of the operative management to prevent ankle stiffness or recurrence of the symptoms. Surgery usually requires a removal of the damaged tissue (debridement) and meticulous repair of the tendon. Post-operative immobilization is required, followed by gradual range of motion and strengthening exercises start. It may require 6 months for the full recovery. Some known complication are recurrence, stiffness of the ankle and deep vein thrombosis.
Prevention
By properly training the body, an athlete can build the strength of their tendons and muscles. Following a workout and dieting plan, the body will be able to build muscle and strengthen most effectively. Additionally, doing the following can prevent tendinitis. Wearing appropriate shoes will give your foot the support it needs for proper movements of the foot and ankle. Improper movements will put additional stress on your body. Stretching before an athletic activity, Stretching primes the body for a taxing activity. Additionally, this will get your blood flowing and reduce the risk of pulling a muscle. Ask your doctor about orthotics, Custom orthotics can help get your foot into proper alignment. If the foot does not execute proper mechanics, the body will adjust which will cause pain and increase the chances of injury.
Achilles-tendinitis is characterized by inflammation and pain at the Achilles tendon (back of the ankle). This tendon, sometimes called the heel cord, is the tendon attachment of the calf muscles from the leg and knee to the heel. This structure is important in standing on your toes or in the pushing-off phase of walking, running, or jumping.Achilles-tendinitis is usually a grade 1 or 2 strain of the tendon. A grade 1 strain is a mild strain. There is a slight pull of the tendon without obvious tendon tearing. (There is microscopic tendon tearing.) There is no loss of strength, and the tendon is the correct length. A grade 2 strain is a moderate strain. There is tearing of tendon fibers within the substance of the tendon or where the tendon attaches to muscle or bone. The length of the tendon or whole muscle-tendon-bone unit is increased, and there is usually decreased strength. A grade 3 strain is a complete rupture of the tendon.
Causes
Although a specific incident of overstretching can cause an Achilles tendon disorder, these injuries typically result from a gradually progressive overload of the Achilles tendon or its attachment to bone. The cause of this chronic overload is usually a combination of factors that can put excess stress on the tendon: being overweight, having a tight calf muscle, standing or walking for a long period of time, wearing excessively stiff or flat footwear, or engaging in significant sports activity.
Symptoms
There are several types of Achilles tendinitis symptoms, but all of them are closely related. People who suffer from Achilles tendon pain typically have swelling in the Achilles tendon, and that pain can be chronic as the microscopic tears in the area become more prevalent over time. The most intense pain is typically located just a few centimeters above the area where the tendon meets the heel. This area is called the watershed zone, and the amount of blood moving through it is what gives it the highest potential for injury, especially for athletes. Most of the Achilles tendinitis symptoms in people with the condition will happen immediately after they have been inactive for a fairly significant amount of time. That means that the most pain will generally be felt after sitting or lying down for an extended period, or right after waking up in the morning and getting moving. If you aren?t positive that you are suffering specifically from Achilles tendinitis symptoms, consult a doctor to make sure.
Diagnosis
A doctor examines the patient, checking for pain and swelling along the posterior of the leg. The doctor interviews the patient regarding the onset, history, and description of pain and weakness. The muscles, tissues, bones, and blood vessels may be evaluated with imaging studies, such as X-ray, ultrasound, or MRI.
Nonsurgical Treatment
There are a variety of treatments for Achilles tendonitis. These range from rest and aspirin to steroid injections and surgery. Your doctor might suggest, reducing your physical activity, stretching and strengthening the calf muscles, switching to a different, less strenuous sport, icing the area after exercise or when in pain, raising your foot to decrease swelling, wearing a brace or compressive elastic bandage to prevent heel movement, undergoing physical therapy, taking anti-inflammatory medication (e.g., aspirin or ibuprofen) for a limited time, getting steroid injections, Sometimes more conservative treatments are not effective. In these cases, surgery may be necessary to repair the Achilles tendon. If the condition intensifies and is left untreated, there?s a greater risk of an Achilles rupture. This can cause sharp pain in the heel area.
Surgical Treatment
Surgery is considered when non-operative measures fail. Patient compliance and postoperative management is an important aspect of the operative management to prevent ankle stiffness or recurrence of the symptoms. Surgery usually requires a removal of the damaged tissue (debridement) and meticulous repair of the tendon. Post-operative immobilization is required, followed by gradual range of motion and strengthening exercises start. It may require 6 months for the full recovery. Some known complication are recurrence, stiffness of the ankle and deep vein thrombosis.
Prevention
By properly training the body, an athlete can build the strength of their tendons and muscles. Following a workout and dieting plan, the body will be able to build muscle and strengthen most effectively. Additionally, doing the following can prevent tendinitis. Wearing appropriate shoes will give your foot the support it needs for proper movements of the foot and ankle. Improper movements will put additional stress on your body. Stretching before an athletic activity, Stretching primes the body for a taxing activity. Additionally, this will get your blood flowing and reduce the risk of pulling a muscle. Ask your doctor about orthotics, Custom orthotics can help get your foot into proper alignment. If the foot does not execute proper mechanics, the body will adjust which will cause pain and increase the chances of injury.